Introduction and Clinical Context
The green sea turtle (Chelonia mydas), hereafter referred to as "Ragool," was admitted as a critical emergency in the advanced stages of hemodynamic collapse. This clinical presentation serves as a living, advanced model of complete metabolic failure and immune anergy in marine reptiles. Such deterioration mandated the immediate activation of an Intensive Care Unit (ICU) Rapid Response protocol. This document represents a pathophysiological dissection of systemic collapse.
The case is highlighted by a dangerous pathological entanglement; endemic mechanical epibiotic biofouling converged with fulminant septic shock triggered by pathogenic entry into the vascular route. Managing this interaction requires deep insight into pharmacokinetics within Debilitated Turtle Syndrome (DTS), alongside the management of catastrophic tissue lysis and widespread ischemia driving the animal toward Multi-Organ Dysfunction Syndrome (MODS).

Initial Comprehensive Physical Diagnostics
Upon admission, initial examination revealed severe deterioration of vital signs, alongside signs of excruciating pain evident in erratic movements and depressive primary neurological reflexes (e.g., nasal and cloacal reflexes). The subject demonstrated signs of clinical shock, clouded consciousness, profound bradypnea, and bradycardia.
Detailed Clinical Manifestations:
| Clinical Sign | Observed Description | Primary Pathophysiological Interpretation |
|---|---|---|
| Fulminant Liquefactive Necrosis | Epithelial and connective tissues suffering from extensive enzymatic lysis (melting skin), synchronous with generalized hemorrhagic erythema. | Advanced septic ulcerative dermatitis (SCUD) driven by proteolytic enzymes, rupturing microvasculature and causing serosanguinous exudate. |
| Hemorrhagic Sub-Scute Edema | Retention of purulent effusions between the eroded osseous layer of the carapace and the superficial keratin plate. | Excessive capillary leak syndrome leading to fluid accumulation, coupled with advanced osteomyelitis. |
| Suppurative Panophthalmitis | Blepharospasm, total closure, accumulation of purulent exudate, and corneal opacity reflecting definite functional blindness. | Severe hypovitaminosis A with ascending hematogenous septic spread to the anterior chamber of the eye. |
Clinical Visual Documentation
Precise exhibition of afflicted segments, dermal lesions, and shell architecture based on macroscopic examination.






Diagnostic Pathomorphology Blueprint
Interactive mapping of primary infection portals and localized macroscopic fractures directly superimposed onto an X-Ray framework simulation mapping (Chelonia mydas). Hover over the anomalous markers to access localized diagnosis.
* Digital representation for ICU anatomical localization.
First Aid & Environmental Stabilization Protocol
Immediately upon reception, the team triggered the "Stabilization Protocol" to prevent further deterioration during advanced diagnostic preparation. The treatment philosophy relies on providing an optimal recovery environment that mimics natural conditions while reinforcing metabolic capacities.
Intensive Care Setup
Accommodated on sterile sponge bases and medical puppy pads. The excoriated skin is immensely fragile and prone to hemorrhage upon any solid contact, making soft padding mandatory.
Total Dry Docking Protocol
Strict isolation from aquatic environments. Complete prevention of water immersion to circumvent catastrophic systemic water aspiration and subsequent respiratory failure.
Thermal Hemodynamic Insulation
Implementation of a controlled hyperthermic environment using medical-grade infrared lamps. Elevating the core temperature deliberately mitigates hypovolemic shock effects and boosts sluggish metabolic clearance.
Among the primary etiology multiplying the clinical collapse was the erroneous intervention by untrained individuals attempting manual, mechanical extraction of epibiotic calcified barnacles prior to admission. Due to their deep vascular integration within live tissue, this blunt trauma generated *Deep Lacerations* and acted as *Open Portals*, inducing direct localized hematogenous dissemination of surface microbiota into the bloodstream, exponentially accelerating comprehensive septicemia.
Pathogenesis & Systemic Sequelae
The pathogenesis (disease development) in Ragool encompasses an acute cascading reaction leading to Systemic Inflammatory Response Syndrome (SIRS). Pathogens infiltrated the dermal barrier, generating virulent endotoxins that provoked widespread vasodilation.
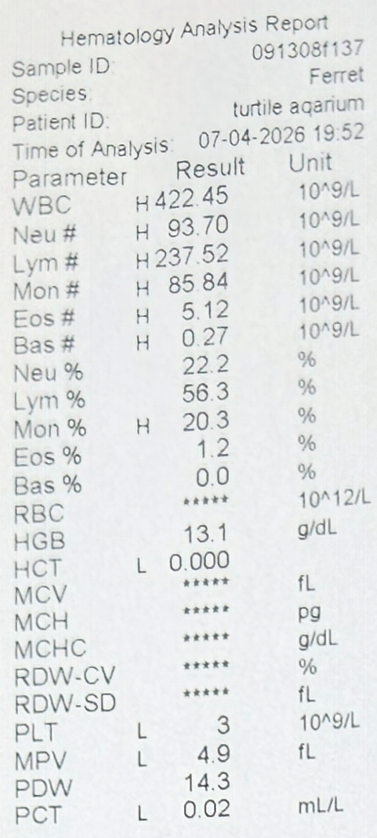
This uncontrolled cascade incited Disseminated Intravascular Coagulation (DIC), where massive depletion of coagulation factors ensued, justifying the diffuse microscopic hemorrhages and abysmal platelet counts (Thrombocytopenia).
The profound immunosuppression directly stems from protracted malnutrition and visceral failure, terminating in functional anergy of macrophages and lymphocytic lines.
Final Prognosis
The medical prognosis for this specimen is officially quantified as "Grave to Guarded". Biological indicators reflect irreversible systemic failure, as the animal lingers within refractory septicemia and expansive tissue necrosis undergoing autolysis despite localized continuation of cardiac faculties.
The specialized response team at the Dept. of International Research - Hurghada Grand Aquarium established a Gold Standard in addressing complex systemic collapse in marine wildlife.